When a patient leaves a primary care physician (PCP) with a specialist referral, a clock starts ticking — and for most healthcare organizations, what happens next is a black hole. The wait is often measured not in days but in weeks. Referrals stall. They get lost. They age silently until what began as an administrative inconvenience has become a clinical risk.
This isn’t a rare edge case. It happens every day, across every specialty, in healthcare organizations of every size. It even has a name: referral aging. Here’s why it happens, what it costs patients, and how modern referral management systems eliminate it.

Photo by Scott Graham on Unsplash
The Anatomy of a Referral That Ages
Referral aging begins the moment a PCP issues a referral and ends — ideally — when the patient sees the specialist and the consult note returns to the referring provider. What happens in between is often invisible to everyone involved.
The numbers are striking. According to AMN Healthcare’s 2025 Survey of Physician Appointment Wait Times, the average patient now waits 31 days for a specialist appointment — a 19% increase from 2022 and a 48% jump since 2004. For certain specialties, the wait is far longer: OB/GYN averages 41.8 days, gastroenterology 40 days, and cardiology 33 days. In some markets, patients wait well beyond two months. Every additional day represents a patient living without a diagnosis or a treatment plan — and a risk profile that grows quietly worse.
Why Referrals Age in the First Place
It’s tempting to attribute referral aging to carelessness or understaffing. The real culprit is structural: most referral workflows simply lack the visibility and accountability needed to catch delays before they compound. Several failure patterns appear consistently across organizations of every size.
Fax-Based Workflows with No Confirmation
Many healthcare organizations still route referrals by fax. A referral is sent — but there is no read receipt, no acknowledgment, no audit trail. It disappears into a void. Intelligent fax automation can eliminate this gap entirely by automatically routing inbound faxes, extracting patient and provider data, and inserting referrals directly into the workflow — with no manual handling required.
Disconnected EHR Systems
Referring physicians and specialists frequently work in different electronic health records that don’t communicate. Neither side sees the full referral lifecycle, and neither knows with certainty whether the referral was received, scheduled, or completed. Without a shared tracking layer, accountability falls through the cracks.
No Defined Follow-Up Ownership
When a referral stalls, it’s often unclear whether the PCP’s office, the specialist’s office, or the patient is responsible for moving it forward. In busy practices, an unowned referral quietly slides down the priority list — until it’s too late.
Patients Who Don’t Know to Follow Up
Patients are typically told they’ll receive a call. When that call doesn’t come, many assume no news means progress. The referral expires while the patient waits. Without automated patient outreach built into the referral workflow, this pattern repeats endlessly.
These failure modes compound each other. The result: referrals that age undetected until the delay itself has become the problem. This is also a primary driver of patient referral leakage — patients who leave the network, don’t complete care, or simply fall through the cracks entirely.
When Waiting Becomes Dangerous
For some referrals, a 31-day wait is an inconvenience. For others, it is catastrophic.
Patients referred for oncology workups, cardiac evaluation, or neurological symptoms face an entirely different risk calculus. In weeks, a disease can progress from a treatable early stage to an advanced one. The window for intervention narrows — and sometimes closes. A landmark systematic review and meta-analysis published in The BMJ found that even a four-week delay in cancer treatment is associated with increased mortality across surgical, systemic treatment, and radiotherapy indications for seven cancer types. A more recent 2025 meta-analysis in GeroScience found that a 12-week treatment delay in colorectal cancer is associated with a 39% higher risk of death compared to timely treatment.
And it’s not just oncology. Even referrals that appear routine can mask urgent underlying conditions. A delayed diagnosis that looks, in hindsight, like a missed opportunity is often traceable not to a clinical error, but to a referral that simply aged out of the queue unnoticed.
According to data from ReferralMD’s referral management platform, 20% of malpractice claims involve missed or delayed diagnoses due to deficits in handoffs between providers. Every untracked referral day is a missed opportunity to diagnose, treat, and prevent avoidable harm. Referral aging is a patient safety issue — and it deserves to be managed as one.
What Effective Referral Management Actually Looks Like
Solving referral aging doesn’t require hiring more staff to manage more paperwork. It requires building a system where every referral has a clear next step, and where delays surface automatically — before they become clinical risk. Here’s what that system looks like in practice.
Workflow Automation
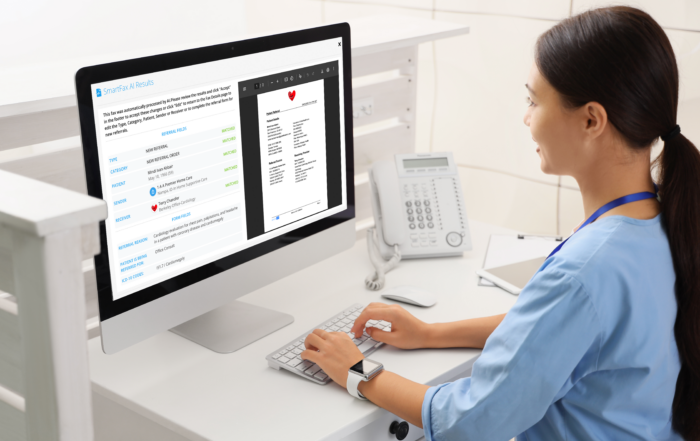
Manual referral tracking consumes enormous staff time: follow-up calls, fax audits, spreadsheet updates, status checks. The staff spends long hours on follow-up calls, checking faxes, updating spreadsheets and invoices. When tracking is automated, staff are redirected toward the cases that genuinely require human judgment — patients who are hard to reach, cases with complex insurance situations, or referrals that need clinical escalation. Automation doesn’t replace people; it frees them for higher-value work. ReferralMD’s SmartFax AI, for example, automatically scans inbound faxes, extracts patient and provider data, categorizes documents, and routes referrals directly into the workflow — turning hours of manual fax processing into seconds.
Real-Time Referral Status Visibility
Every referral should have a live, visible status accessible to both the referring and receiving provider. This eliminates guesswork and constant phone tag. A well-configured system can flag an urgent oncology referral that hasn’t been scheduled within 48 hours — and trigger a lower-priority reminder for routine referrals after 10 days. Nothing gets lost. Issues are surfaced when they’re still easy to resolve.
Automatic Closed-Loop Closure
Many practices consider a referral “done” the moment it’s sent. But sending is just the beginning. A referral should remain open in the system until two things happen: the appointment occurs, and the specialist’s consult note returns to the referring provider. Until that moment, the patient’s care episode is clinically incomplete. A closed-loop referral platform enforces this standard automatically — ensuring that every referral has a documented outcome, not just a sent status.
Patient-Facing Engagement Tools
A significant share of referral delays happen on the patient side. People wait for a call that never comes, miss scheduling windows, or give up navigating complex intake processes. Automated SMS and email reminders, self-scheduling links, and frictionless rescheduling options reduce drop-offs meaningfully. When completing a referral takes under a minute from a patient’s phone, completion rates improve — and fewer patients fall through.
Live Dashboards with Age-Based Alerts
High-performing health systems use dashboards that organize every open referral by age bucket — 0–7 days, 8–14 days, 15+ days — with visual alerts that escalate by clinical urgency. These dashboards make it possible to spot bottlenecks, redistribute volume proactively, and hold teams accountable to completion benchmarks. Unlike monthly reports, live dashboards enable real-time course correction. When a high-risk referral hasn’t moved in 48 hours, the system catches it — not a retrospective audit three weeks later.
The Bottom Line
Referral aging puts patients at real clinical risk — but it is a solvable problem. The technology to automate referral tracking, surface delays in real time, close loops automatically, and engage patients proactively exists today. Organizations that implement it don’t just improve operational efficiency; they reduce clinical risk, strengthen network integrity, and ensure that the care patients were referred for is care that actually happens.
Want to see how ReferralMD eliminates referral aging across your network? Request a demo.
About the Author: Brooke Webber is a marketing and sales content specialist focused on people-first strategies that connect brand messaging with real customer needs. Her areas of focus include buyer psychology, customer experience, and revenue-driven communication, with five years of writing experience across B2B industries.
Related Posts
Subscribe to Our Blog
Recent Posts