Bridging the Digital Divide: Strategies for Making Health Tech Accessible to All Patients in 2026
We still describe the digital divide as a technology problem. In healthcare, it shows up differently.
A missed login becomes a missed diagnosis.
A weak signal becomes a delayed treatment.
A lack of access turns into another unnecessary trip across town.
Image source: Freepik
Healthcare technology is now embedded in patient access. Virtual care, remote monitoring, referral management systems, and patient portals. These are no longer optional layers. They are part of how care is delivered.
If patients cannot use them, they are not in the system.
This article looks at where the gaps actually sit today and what it takes to close them, across infrastructure, cost, skills, and design, not in theory, but in practice.
Understanding the Digital Divide in Healthcare
The digital divide in healthcare is not a single barrier. It’s a stack of small failures that compound. A rural clinic loses a video consult because bandwidth drops mid-visit. A parent joins a behavioral health session on a prepaid phone and keeps reconnecting. An older adult gives up after repeated login errors. A patient opens instructions that were never written for them.
Each situation looks manageable on its own. Together, they determine whether care happens at all. Connectivity, cost, skills, and design don’t operate independently. When one breaks, the rest rarely compensate.
Access improved quickly after 2020, but it didn’t level out. The surge in telehealth didn’t close the gap. It made it visible.
A portion of the population remains completely offline. About 7% of adults didn’t use the internet at all, with older and lower-income populations disproportionately represented.
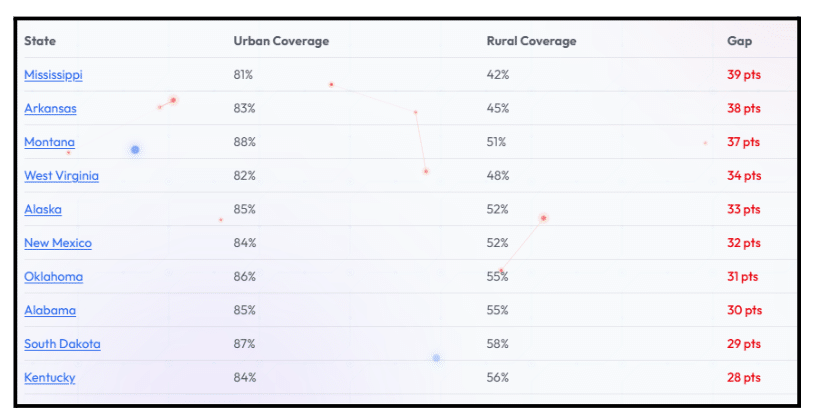
Geography continues to shape access in more subtle ways. Urban areas average 4.1 providers offering 100/20 Mbps service, while rural areas average just 1.4. In Mississippi, broadband access drops from 81% in urban areas to 42% in rural regions. That gap shows up in real use. Lag, dropped calls, and inconsistent connections directly affect care delivery.
The Importance of Bridging the Digital Divide
When access improves, care changes.
Patients catch issues earlier. Fewer unnecessary ER visits. Follow-ups actually happen. Care teams coordinate faster. On the system side, missed appointments drop and capacity stretches further.
For patients, it’s simpler than that. Less travel. Less waiting. Less friction.
There’s already momentum. Workflows have been redesigned. Patients have adapted to hybrid care. The next step is making sure those gains reach people who weren’t included the first time.
Key Barriers to Digital Health Access
These barriers don’t show up one at a time. They overlap. That’s why fixing just one rarely works. Here are the ones that consistently block patient experience in real settings:
1. Infrastructure issues
In some communities, the problem is still basic: the connection isn’t reliable enough to support care.
Video visits freeze. Data uploads fail. Remote monitoring devices lose sync. Clinics trying to deliver care through advanced healthcare technology often end up adjusting workflows around unstable networks instead of clinical needs.
The issue isn’t just speed; it’s consistency. A connection that works one day and fails the next is enough to erode trust in digital care entirely.
2. Economic barriers
Even where infrastructure exists, cost limits who can use it.
Devices aren’t cheap. Data plans aren’t either. The Affordable Connectivity Program (ACP) helped offset that for many households, but funding began to wind down in 2024, as noted in a Congressional Research Service report. What remains is uneven and often temporary.
For patients managing chronic conditions, this becomes a recurring tradeoff. Do they prioritize connectivity or other essentials? That decision directly affects engagement with healthcare systems.
Cost doesn’t just delay access. It narrows it.
3. Digital literacy
Access without usability doesn’t translate into care.
Patients are expected to navigate portals, connect devices, manage passwords, and recognize security risks. These are learned skills and not evenly distributed.
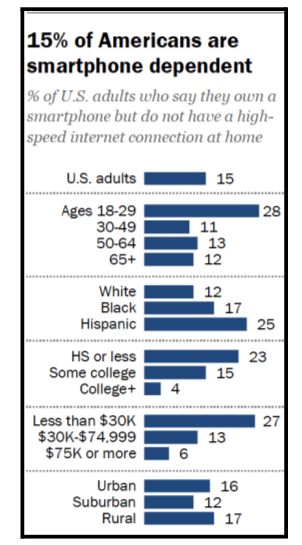
Around 15% of U.S. adults were “smartphone-only” users. For many, that means managing care on a small screen, with limited data, and unstable connections. Try uploading documents, reviewing results, or completing forms that weren’t designed for mobile. It works, until it doesn’t.
That limitation compounds when systems assume a higher level of digital comfort. During the pandemic, research showed that digital literacy strongly influenced telehealth use and equity.
But the barrier isn’t just knowledge. It’s hesitation.
When someone isn’t confident using a tool, they avoid it—missed logins become missed visits. Small friction points compound into disengagement.
4. Cultural and language barriers
Design choices quietly determine who gets included.
Instructions written in complex English. Interfaces built around assumptions of digital familiarity. Limited support for accessibility features like captions or screen readers.
Even where telehealth adoption increased, it didn’t look the same across communities. According to the National Center for Health Statistics survey in 2021, usage ranged from about 32% to 33% among Hispanic, non-Hispanic Black, and non-Hispanic Asian adults, compared with about 39% among non-Hispanic White adults and over 40% among American Indian or Alaska Native adults. These differences point to how cultural context, language, and trust shape whether digital care is actually used.

Those gaps often reflect more than access. They reflect whether systems were designed in a way that patients could actually use.
Not because patients don’t want care. Because the system wasn’t built for them.
Strategies to Make Health Tech Accessible
Closing the gap isn’t about adding more tools. It’s about making existing systems usable in real conditions. Here are the approaches that consistently move the needle:
1. Improving infrastructure
Large-scale investment is underway. The Broadband Equity, Access, and Deployment (BEAD) program is allocating more than $42 billion to expand high-speed internet.
But infrastructure rollout takes time.
In the meantime, clinics are adapting. Fixed wireless, 5G home internet, and low Earth orbit satellite services are being used as interim solutions in areas where fiber isn’t yet viable.
Design decisions matter just as much. Systems that support low bandwidth, offer audio-only options, or allow asynchronous communication keep care accessible even when connectivity isn’t ideal.
This is where healthcare IT professionals play a critical role, shaping systems that can operate under real-world constraints rather than ideal conditions.
That’s often what determines whether a visit happens.
2. Economic interventions
Cost barriers don’t disappear on their own. They have to be designed around. Devices, data plans, and monitoring tools all add up, and for many patients, that cost sits outside traditional care coverage.
The most effective approaches reduce the upfront burden. Device lending, subsidized connectivity, and shared funding models allow patients to participate without committing to ongoing costs they may not be able to sustain.
Screening for affordability makes these efforts more consistent. Simple intake questions help identify who needs support, and clinics can connect patients to local programs, digital navigator services, or remaining subsidy options.
Having worked closely with teams implementing digital solutions in cost-sensitive environments, Christopher Skoropada, CEO of Appsvio, has seen how financial barriers shape real-world adoption.
“I’ve seen that access often breaks down at the cost level before anything else. Even when the technology is available, patients won’t engage if the setup feels like an added expense. The systems that work are the ones that lower that initial barrier and make participation feel manageable from the start,” Skoropada notes.
3. Enhancing digital literacy
Digital literacy improves when support is immediate and practical.
Short, hands-on guidance works better than written instructions. Patients benefit from walking through setup steps before their appointment, not during it.
Community health workers and peer educators play a critical role here. They don’t just explain how tools work. They make them feel usable.
Support materials still matter, but they need to be simple. Clear screenshots. Minimal steps. Plain language. Short videos in multiple languages.
Help desk availability also matters. If support isn’t available when patients need it, they stop trying.
4. Culturally sensitive approaches
Accessibility requires more than translation.
Health systems are aligning with CLAS standards to guide culturally and linguistically appropriate care. At the same time, WCAG guidelines are shaping how digital tools support different accessibility needs.
But beyond standards, flexibility matters.
Some patients prefer SMS reminders. Others rely on phone calls. Some are comfortable with apps; others are not. Offering multiple pathways allows patients to engage at their own pace.
Adoption improves when patients aren’t forced into a single way of interacting with care.
Case Studies and Examples
Some systems have already operationalized these ideas in ways that hold up beyond pilot stages. The difference isn’t the tools themselves. It’s how access is built into care delivery.
Here are a few examples:
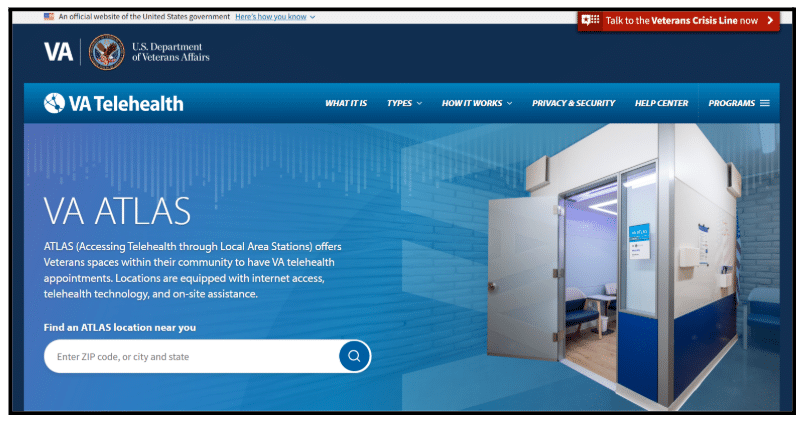
1. Telehealth access points in community settings
The U.S. Department of Veterans Affairs developed the ATLAS program, placing telehealth-enabled sites in community locations. These sites provide devices, connectivity, and private spaces for care, allowing patients without home internet to attend virtual appointments reliably.
2. Device-supported care with structured clinical oversight
Ochsner Health has taken a more integrated approach. Through its digital medicine programs, patients receive connected devices alongside structured clinical support.
Reported outcomes show that 80% of patients with hypertension achieved blood pressure control within six months, while 73% of patients with diabetes reached target A1C levels. The combination of devices and ongoing support extends care beyond the clinic, making remote management more consistent.
3. Libraries as telehealth hubs
Community-based models are also gaining traction. Health centers partnering with libraries and local organizations are embedding digital navigators to support patients with connectivity enrollment, device setup, and ongoing use, reflecting a broader shift toward libraries as telehealth hubs.
This approach improves readiness for virtual care and has been implemented across multiple communities as part of broader digital inclusion efforts.
Across these examples, the pattern is consistent. Access is treated as part of care delivery, not a separate initiative.
Future Trends in Health Tech Accessibility
Several shifts are already underway, and their impact will depend on how they’re implemented.
Kashif Ali, Growth Specialist at PsychologySchoolGuide.net, studies how people actually engage with digital tools in real-world settings, where usability and accessibility often determine whether systems are used at all.
He says, “I’ve seen that access alone doesn’t lead to adoption. People engage more when systems feel intuitive from the start and guide them clearly through each step. The tools that gain traction are the ones that reduce friction early, especially for those who are less comfortable with technology.”
Connectivity options are also expanding. Fixed wireless and satellite providers are increasing competition in rural and suburban markets, which may improve both pricing and availability over time.
Devices are becoming easier to use. Setup processes are simpler, battery life is improving, and more systems are moving toward plug-and-play configurations that reduce reliance on smartphones.
Software is evolving as well. Real-time translation, voice-based navigation, and simplified instruction layers are starting to reduce barriers for patients with limited digital literacy.
On the systems side, interoperability efforts like TEFCA are improving data exchange. This reduces friction in care coordination, where delays often stem from disconnected systems.
Payment models are also shifting. Value-based care contracts are beginning to include measures tied to equitable access, not just overall outcomes.
Where to Start
Bridging the digital divide doesn’t start with a large-scale transformation. It starts with small, deliberate steps.
Add connectivity questions to the intake. Identify patients who may struggle to access care. Build referral management. Pilot a device lending program for a specific condition and measure the results.
Design systems that work under real conditions. Low bandwidth. Limited devices. Different levels of familiarity.
Then track what happens.
Because access to digital care shouldn’t depend on where someone lives, what they can afford, or how comfortable they are with technology.
Author’s Bio: Catherine is a marketing & e-commerce specialist who helps brands grow their revenue and move their businesses to new levels.
Related Posts

Subscribe to Our Blog
Recent Posts